 The really bad news is that we have elected a misogynistic felon with a narcissistic personality disorder. Even worse news is that people have fallen for Trump’s lies.
The really bad news is that we have elected a misogynistic felon with a narcissistic personality disorder. Even worse news is that people have fallen for Trump’s lies.
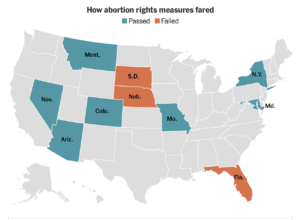
There’s some good news, despite lots of disappointments. In my state, Colorado, almost 2/3rds of voters chose to amend our constitution to guarantee the right to safe abortion care. In addition, the state will start paying for abortions for women who are state and local government employees, and for those on Medicaid.
The state to our north, Wyoming, had abortion laws preventing almost all abortions. In November, a Wyoming judge ruled that the laws were against that state’s constitution. She wrote: “The abortion statutes suspend a woman’s right to make her own health care decisions during the entire term of a pregnancy and are not reasonable or necessary to protect the health and general welfare of the people.” Although the state will probably appeal this decision, for now women can obtain safe, legal abortion care in Wyoming.
Public health scientists have identified several causes why young children don’t flourish. Children may not do well if pregnancies are too close together. We also know that if a mother really, really doesn’t want to carry a pregnancy, but is forced to give birth, that the child may not fare well. Do children who result from unintended pregnancies also suffer?
“Yes” is the sad answer. Researchers looked at Demographic and Health Surveys from developing countries. Surveyed mothers rated their births as being desired, mistimed or unwanted. The endpoint of the research was infant mortality—the death of the child before age one year of age. What they found is that children whose pregnancies were described as unwanted or mistimed were more likely to die. This finding held for 41 of the 60 countries studied. Moreover, the effect was stronger in poorer, less educated places.
Unfortunately, there are over 120 million unintended pregnancies globally each year. These findings are the bad news. The good news is that now there is proof that contraception decreases infant mortality in impoverished areas.
Unfortunately, there is concerning news about two of the Long-Acting Reversible Contraceptive (LARC) methods. DepoProvera, has been associated with an increased risk of users developing meningiomas. These are benign tumors of the membranes covering the brain. Meningiomas are more common in women, and have been found to have receptors that respond to female hormones. However, the risk of developing a meningioma is very, very small, and it is still very small for users of Depo.
There are four IUDs containing a hormone. In addition to providing excellent contraception, they make periods less painful and lighter. Fortunately, they don’t seem to increase the risk of meningioma, but the latest information is that they may increase the risk of breast cancer.
It will take more studies to confirm (or refute) these concerns about LARCs causing tumors. In the meantime, it is the right of women to know of these possibilities. However, the risks of morbidity or mortality from pregnancy exceed by far the likelihood of a problem caused by any contraceptive method, if used properly. For women who desire long-term reversible birth control, the ParagardÒ IUD is a hormone-free LARC. It can provide excellent protection for 10 years—or possibly even longer.
Since the Dobbs decision, many states have made it very difficult to access safe abortion care. Furthermore, unintended pregnancies cause problems if the mother is forced to carry to term. Taken together, these facts make it all the more important to increase the availability of contraception.
©Richard Grossman MD, 2024
